Hip Resurfacing Arthroplasty
|
||||||


Introduction
Physiotherapy in Edmonton for Hip
Welcome to In Step Physical Therapy's resource with respect to Hip Resurfacing Arthroplasty.
A hip that is painful as a result of osteoarthritis (OA) can severely affect your ability to lead a full, active life. Over the last 25 years, major advancements in hip replacement have greatly improved the outcome of the surgery.
Hip resurfacing arthroplasty is a type of hip replacement that replaces the arthritic surface of the joint but removes far less bone than the traditional total hip replacement. Because the hip resurfacing removes less bone, it may be preferable for younger patients that are expected to need a second, or revision, hip replacement surgery as they grow older and wear out the original artificial hip replacement.
This guide will help you understand:
- what your surgeon hopes to achieve
- what happens during the procedure
- what to expect after your operation
Anatomy
What parts of the hip are involved?
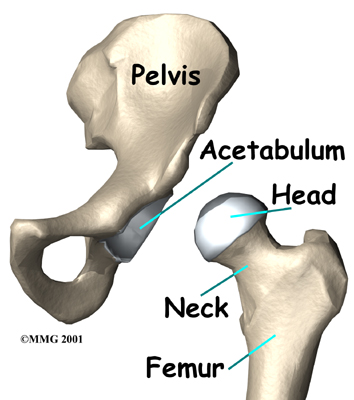
The hip joint is one of the true ball-and-socket joints of the body. The hip socket is called the acetabulum and forms a deep cup that surrounds the ball of the upper thighbone, known as the femoral head. Hip resurfacing may only affect the head of the femur or it may involve both the femoral head and the hip socket.
Related Document: In Step Physical Therapy's Guide to Hip Anatomy
Rationale
What does the surgeon hope to achieve?
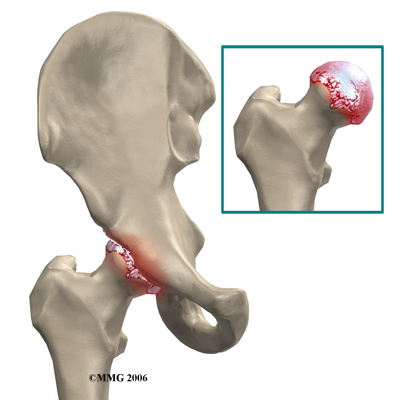
The main reason for replacing any arthritic joint with an artificial implant is to stop the bones from rubbing against each other. This rubbing causes pain. Replacing the painful and arthritic joint with a new surface, allows the joint to move smoothly without pain. The goal is to help people return to many of their activities with less pain and greater freedom of movement.
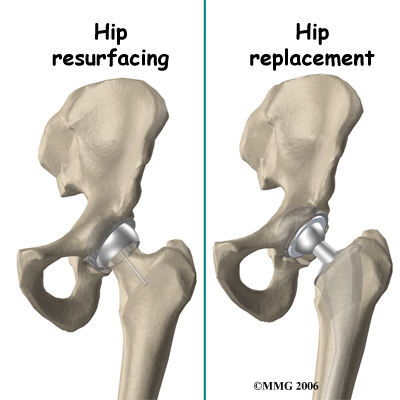
The most important reason to do a hip resurfacing rather than a traditional artificial hip replacement, is to remove as little bone around the hip as possible. This is especially important when you may need a second, or revision, hip replacement as you grow older.
The most common cause for revision of an artificial hip is loosening of the pieces of the artificial hip joint where it attaches to the bone. The loosening process results in wearing away of the bone around the metal components, or parts of the artificial joint. This is especially true around the stem of the femoral component that fits inside of the femoral shaft in the traditional artificial joint. The femoral component used during hip resurfacing is placed on the outside of the femoral head and the femoral shaft is never disturbed. This means that when a revision is needed, the femoral shaft can be used to hold the femoral component as if there has never been an artificial joint and the bone in this area is virginal.
Preparation
How should I prepare for surgery?
The decision to proceed with surgery should be made jointly by you and your surgeon only after you feel that you understand as much about the procedure as possible. Many patients wonder when they should consider surgery. Most surgeons agree that surgery is advised when a patient’s pain and discomfort limit daily life and activities.
Once the decision to proceed with surgery is made, several things may need to be done. Your orthopedic surgeon may suggest a complete physical examination by your medical or family doctor. This is to ensure that you are in the best possible condition to undergo the operation. You may also need to spend time with the physiotherapist who will be managing your rehabilitation after the surgery.
One purpose of the preoperative physiotherapy visit is to record a baseline of information. This includes measurements of your current pain levels, functional abilities, and the movement and strength of each hip.
A second purpose of the preoperative therapy visit is to prepare you for your upcoming surgery. You will begin to practice some of the exercises you will use just after surgery.
You will also be trained in the use of crutches or a walker. Your physiotherapist will also assess any needs you will have at home or work once you're released from the hospital.
You may be asked to donate some of your own blood before the operation. This blood can be donated three to five weeks before the operation, and your body will make new blood cells to replace the loss. At the time of the operation, if you need to have a blood transfusion you will receive your own blood back from the blood bank.
Surgical Procedure
Surgeons perform this operation using several different incisions, or approaches, to the hip joint. The anterior approach from the front of the hip and the posterior approach from the back of the hip. There is no one right approach. Many surgeons prefer the posterior approach because it keeps the joint capsule intact. Keeping the joint capsule intact may reduce the risk of dislocation after the surgery and damage the blood supply less. Either approach is commonly used depending on the training and experience of the surgeon.
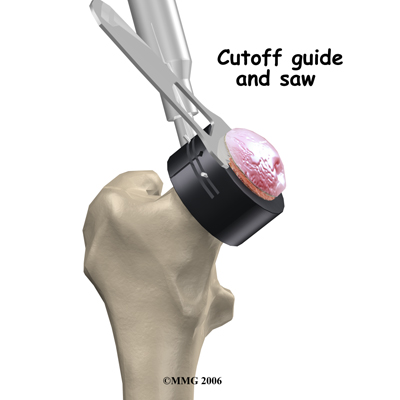
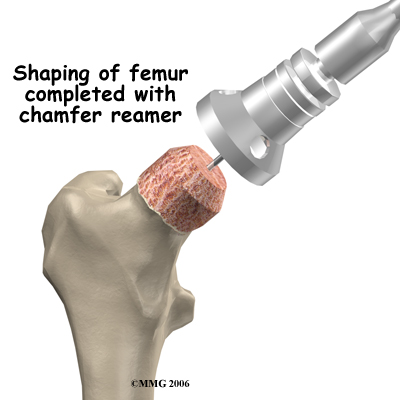
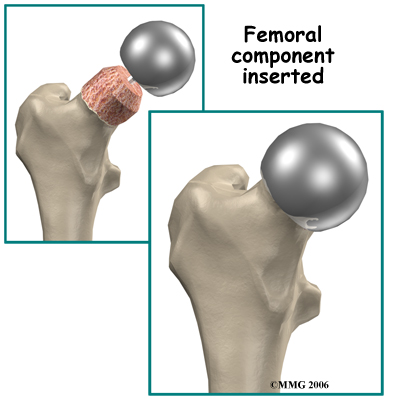
The operation begins by making an incision in the side of the thigh. This allows the surgeon to see both the femoral head and the acetabulum (or socket). The femoral head is then dislocated out of the socket. Special powered instruments are used to shape the bone of the femoral head so that the new metal surface will fit snugly on top of the bone.
Shape the Bone
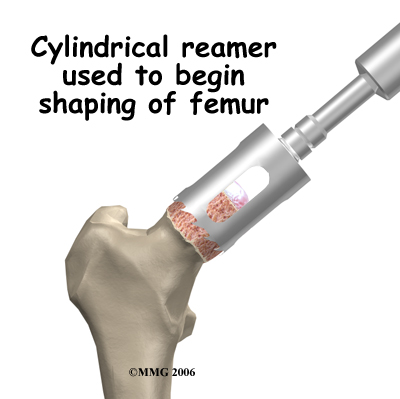
Femoral Head
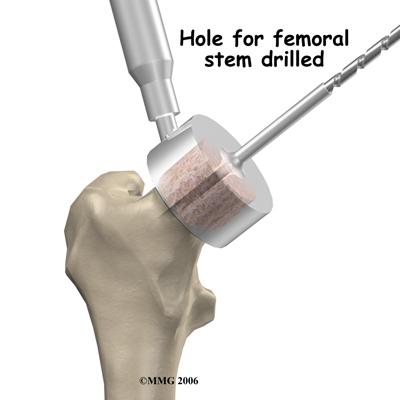
The cap is placed over the smoothed head like a tooth capped by the dentist. The cap is held in place with a small peg that fits down into the bone.
Small Peg
The patient must have enough healthy bone to support the cap.
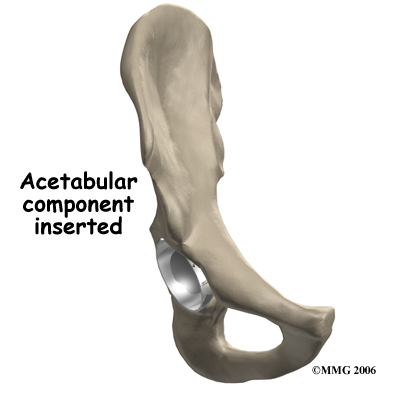
The hip socket may remain unchanged but more often it is replaced with a thin metal cup. A special tool called a reamer is used to remove the cartilage from the acetabulum and shape the socket to fit the acetabular component. Once the shape is correct, the acetabular component is pressed into place in the socket. Friction holds the metal liner in place until bone grows into the holes in the surface and attaches the metal to the bone.
Reamer
Complications
What could go wrong?
As with all major surgical procedures, complications can occur. This document doesn't provide a complete list of the possible complications, but it does highlight some of the most common problems. Some of the most common complications following hip resurfacing arthroplasty surgery include:
- anesthesia complications
- thrombophlebitis
- infection
- dislocation
- femoral neck fracture
- leg length inequality
- loosening
Anesthesia Complications
Most surgical procedures require that some type of anesthesia be done before surgery. A very small number of patients have problems with anesthesia. These problems can be reactions to the drugs used, problems related to other medical complications, and problems due to the anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
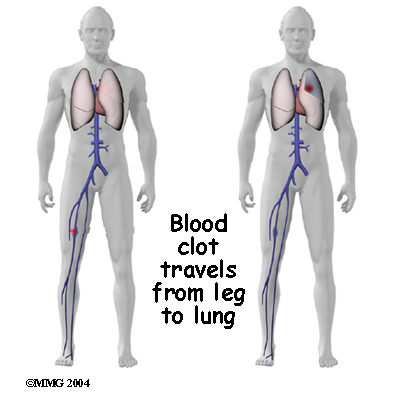
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation, but it is more likely to occur following surgery on the hip, pelvis, or knee. DVT occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include:
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Infection can be a very serious complication following artificial joint replacement surgery. The chance of getting an infection following hip joint resurfacing is probably around one percent. Some infections may show up very early, even before you leave the hospital. Others may not become apparent for months, or even years, after the operation. Infection can spread into the artificial joint from other infected areas. Your surgeon may want to make sure that you take antibiotics when you have dental work or surgical procedures on your bladder or colon to reduce the risk of spreading germs to the joint.
Dislocation
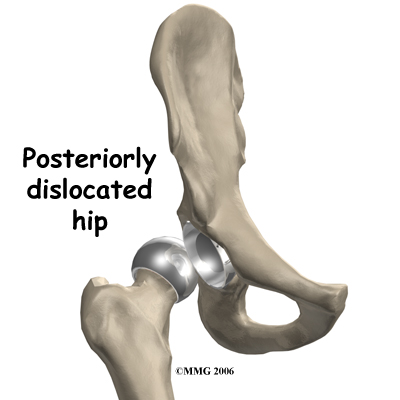
Just like your real hip, an artificial hip can dislocate if the ball comes out of the socket. There is a greater risk just after surgery, before the tissues have healed around the new joint, but there is always a risk. The physiotherapist will instruct you very carefully how to avoid activities and positions that may have a tendency to cause a hip dislocation. A hip that dislocates more than once may have to be revised to make it more stable. This means another operation.
Related Document: In Step Physical Therapy's Guide to Artificial Hip Dislocation Precautions
Loosening
The main reason that artificial joints eventually fail continues to be the loosening of the metal or cement from the bone. Great advances have been made in extending how long an artificial joint will last, but most will eventually loosen and require a revision. Hopefully, you can expect 12 to 15 years of service from an artificial hip, but in some cases the hip will loosen earlier than that. A loose hip is a problem because it causes pain. Once the pain becomes unbearable, another operation will probably be required to revise the hip.
Related Document: In Step Physical Therapy's Guide to Revision Arthroplasty of the Hip
Fracture of the Femoral Neck
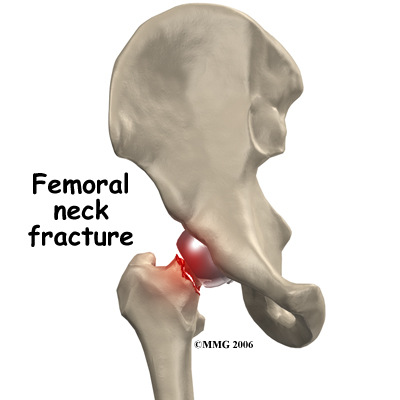
Fracture of the femoral neck is a unique complication of hip resurfacing. The replacement cap fits over the femoral head and ends just about where the femoral neck begins. This meeting point is an area of increased stress risk. Patient obesity, decreased bone mass, and surgical error are common risk factors in femoral neck fracture.
Leg Length Inequality
If there is any bone loss a difference in leg length can occur. When a surgeon does a traditional artificial hip replacement, the leg can be lengthened or shortened to match the other side. Because much less bone is removed during hip joint resurfacing, the surgeon cannot adjust the length of the leg. If you have a leg length difference before the procedure it will remain essentially the same.
After Surgery
What happens after surgery?
After surgery, your hip will be covered with a padded dressing. Special boots or stockings are placed on your feet to help prevent blood clots from forming. A triangle-shaped cushion may be positioned between your legs to keep your legs from crossing or rolling in.
If your surgeon used a general anesthesia, a nurse or respiratory therapist will visit your room to guide you in a series of breathing exercises. You'll use a breathing device known as an incentive spirometer to improve breathing and avoid possible problems with pneumonia.
Physiotherapy treatments are scheduled one to three times each day as long as you are in the hospital. Your first session is scheduled soon after you wake up from surgery. Your therapist will begin by helping you move from your hospital bed to a chair. By the second day, you'll begin walking longer distances using your crutches. Most patients are safe to put comfortable weight down when standing or walking. However, if your surgeon used an uncemented prosthesis, you may be instructed to limit the weight you bear on your foot when you are up and walking.
Your therapist will review exercises to begin toning and strengthening the thigh and hip muscles. Ankle and knee movements are used to help pump swelling out of the leg and to prevent the formation of blood clots.
This procedure requires the surgeon to open up the hip joint during surgery. This puts the hip at some risk for dislocation after surgery. To prevent dislocation, patients follow strict guidelines about which hip positions to avoid (called hip precautions). Your therapist will review these precautions with you during the preoperative visit and will drill you often to make sure you practice them at all times for at least six weeks. Some surgeons give the OK to discontinue the precautions after six to 12 weeks because they feel the soft tissues have gained enough strength by this time to keep the joint from dislocating.
Related Document: In Step Physical Therapy's Guide to Artificial Hip Dislocation Precautions
Patients are usually able to go home after spending two to four days in the hospital. You'll be on your way home when you can demonstrate a safe ability to get in and out of bed, walk up to 75 feet with your crutches or walker, go up and down stairs safely, and consistently remember to use your hip precautions. Patients who still need extra care may be sent to a different hospital unit until they are safe and ready to go home.
Your staples will be removed two weeks after surgery.
Most orthopedic surgeons recommend that you have checkups on a routine basis after your joint resurfacing. How often you need to be seen varies from every six months to every five years, according to your situation and what your surgeon recommends.
Patients who have a joint implant will sometimes have episodes of pain, but if you have pain that lasts longer than a couple of weeks, you should consult your surgeon. During the examination, the orthopedic surgeon will try to determine why you are feeling pain. X-rays may be taken of your hip to compare with the ones taken earlier to see if there is any evidence of fracture or loosening.
Portions of this document copyright MMG, LLC.
Our Rehabilitation
What should I expect during my recovery?
After you are discharged from the hospital, your physiotherapist at In Step Physical Therapy may see you for outpatient visits. This is to ensure you are safe in and about the home and workplace and getting in and out of a car. We will review your exercise program, continue working with you on your hip precautions, and make recommendations about your safety. Our physiotherapist may use heat, ice, or electrical stimulation to reduce any swelling or pain.

You should use your crutches or cane(s) as instructed. Your surgeon may only want you to place the toes of your operated leg down for up to six weeks after surgery. You'll advance the weight you place through your sore leg as tolerated.
Although the time required for recovery varies, patients are usually able to drive within three weeks and walk without a walking aid by six weeks. Upon the approval of our physiotherapist, patients are generally able to resume sexual activity by one to two months after surgery.
Our physiotherapists sometimes treat our patients in a pool. Exercising in a swimming pool puts less stress on the hip joint, and the buoyancy lets you move and exercise easier. Once you've gotten your pool exercises down and the other parts of your rehab program advance, you may be instructed in an independent home program.
When you are safe in putting full weight through the leg, our physiotherapist can choose several types of balance exercises to further stabilize and control the hip.
Many patients have less pain and better mobility after having hip resurfacing. Our physiotherapist will work with you to help keep your new joint healthy for as long as possible. This may require that you adjust your activity choices to keep from putting too much strain on your new hip joint.
There is a belief that with hip resurfacing the patient can return to full participation in recreational or professional sports. Long-term results have not been studied to support this idea. Most surgeons agree that joint resurfacing allows patients to be more active than is acceptable for a standard total hip replacement.
Although resurfacing materials are strong, they aren’t immune to wear and tear. Our physiotherapists usually advise patients to avoid high-impact activities. Heavy sports that require jogging, running, jumping, quick stopping and starting, and cutting are discouraged. Repetitive impact can strain the resurfacing, increasing the risk of loosening.
At In Step Physical Therapy our goal is to help you maximize strength, weight shift evenly, walk normally, and improve your ability to do your activities. When your recovery is well under way, regular visits to our office will end. Although, we will continue to be a resource, you will be in charge of doing your exercises as part of an ongoing home program.
In Step Physical Therapy provides services for physiotherapy in Edmonton.
